Knee
Read more about conditions we treat and surgical procedures we perform on the knee.
ACL Reconstruction
The anterior cruciate ligament (ACL) is important in the knee for stabilisation of the knee in twisting movements. This is particularly relevant in sports that require pivoting and changes in direction (like football, netball and soccer).
Unfortunately, accidents in these sports can result in tears of this ligament. A knee reconstruction should be considered for active patients who want to resume sport again, as engaging in these sports without an anterior cruciate ligament can result in the knee giving way with damage to the articular cartilage and menisci of the knee.
An ACL reconstruction is performed by using part of the patient’s hamstring or patella tendon and fixing this in the position of the original ACL. The procedure is done arthroscopically and most patients stay one night in hospital and can weight bear on the leg right away with the use of crutches.
It is important to strengthen the knee correctly to recover from an ACL reconstruction and patients are usually placed in a knee splint until they get quadriceps control of the knee. In the meantime, the main aim for the first 6 weeks is to regain range of motion of the knee with some strengthening.
Activities like cycling and swimming are allowed after 6 weeks. The next few months are directed towards strengthening the knee to cope with increasing activity. The patient is allowed to jog after about three months and return to sport at 9-12 months post-operatively. This process should be guided by a skilled musculoskeletal physiotherapist to ensure a safe return to pre-injury activity.
General complications to ACL reconstruction are rare but may include:
- numbness in the surgical scar area.
- infection in the surgical incisions
- damage to structures, nerves, or blood vessels around and in the knee
- blood clots in the leg
- the usual risks of anaesthesia
- problems with the graft tendon (loosening, stretching, re-injury, or scar tissue)
- knee joint stiffness
- pain or dysfunction of the patella-femoral joint (the joint between your knee cap and leg bone). This can be addressed with the correct set of exercises
The experienced surgical team uses special techniques to minimise all the above risks. Adverse events following knee surgery are extremely rare, but they cannot be completely eliminated.

What to expect
How long will I be in hospital?
This is usually an overnight stay.
How many stitches will I have?
The small arthroscopic cuts will be closed with a dissolving stitch under the skin and covered with tapes over the wound to reinforce the wound.
What do I do with my dressings?
A bulky, firm dressing is applied directly after your surgery to minimise bruising and haematoma formation. This can be removed 24 hours after your surgery. The waterproof dressing underlying this can get wet in the shower but should be left intact until your post operative review 10 to 14 days post surgery. If this latter dressing becomes loose, a fresh, waterproof dressing should be applied to cover the wound until your post operative review.
Can I walk after the operation?
Most people are fully weight bearing straight after the operation. Some require crutches to help for a short period of time. A knee splint may be required until straight leg raising is possible. The aim is to cease the splint as soon as possible.
What are the risks of this operation?
This operation, as with any others, requires an anaesthetic which in a fit, healthy young person is relatively straight forward. Specific anaesthetic risks will be discussed with your anaesthetist.
There is a small risk of infection following this operation and antibiotics are given during the peri-operative period to minimise this risk.
A blood clot in the veins of the calf is a potential risk but a blood thinning injection will be given to you at the time of your operation to thin the blood enough to minimise this risk. If a blood clot should form, break off and go to the lungs, it can be serious and you must report any shortness of breath, coughing up of blood or severe chest pain. These are the signs of a pulmonary embolus.
When can I play sport after this operation?
Twisting sports are contraindicated for at least 9 months following an anterior cruciate ligament reconstruction but straight line sports can begin in consultation with your surgeon and physiotherapist within 2 to 3 months of your operation. These include jogging in straight lines, cycling, swimming etc.
When should I start my physiotherapy?
Physiotherapy should be started as soon as possible, usually within the first week, when the knee feels comfortable enough to begin some gentle exercises.
When may I drive?
This depends a little bit on which leg was operated on and whether you have an automatic or manual car. The key to the decision on driving is whether you can safely stop in an emergency situation. Your surgeon and physiotherapist can guide you as to when this may be safe. You can also be guided by sitting in a stationary vehicle in your driveway, imagining an emergency situation and attempting to make the appropriate avoidance procedures. If this is uncomfortable, you will know it is not safe to begin driving at this stage.
Please do not attempt to drive at all in the first two weeks post surgery.
What graft material will be used?
Graft material is usually the middle third of the patella tendon connecting the knee cap to the shin bone or hamstring tendon taken from the inside of the knee. Your surgeon will answer questions about graft choice.
How is my graft fixed in position?
An Endobutton (metal fixateur) is fixed to the graft at the femoral (thigh bone) end and an interference screw (usually biodegradable) is used to fix the graft in the tibial (shin bone) tunnel.
How long will I be off work?
This will depend on the type of work you do. If you work in an office, you may return when you feel comfortable but we would suggest 1 – 2 weeks off work. If you do physical work you may need 4-6 weeks off work.
Knee Scope
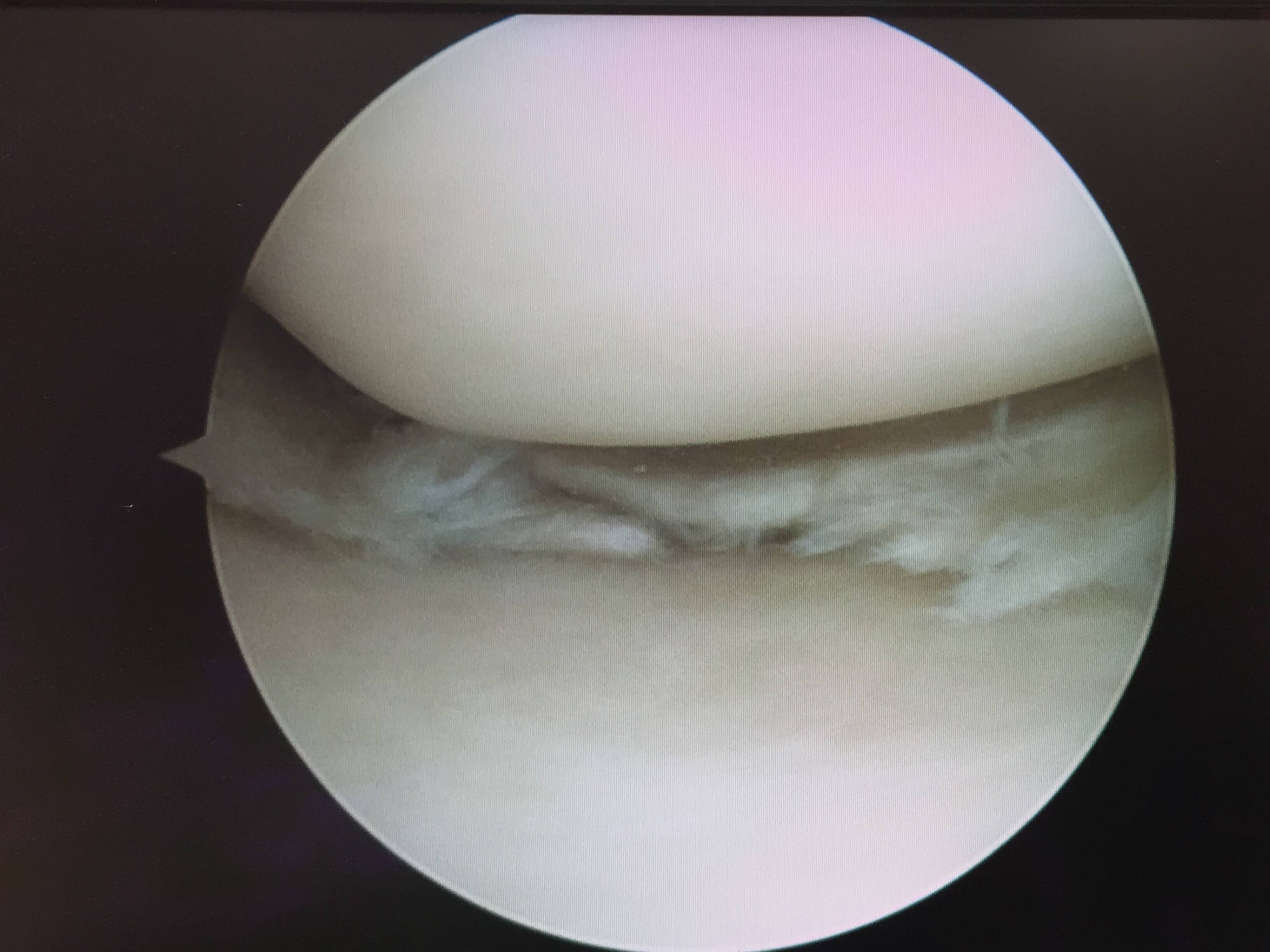
The menisci structures are made of cartilage that act as “shock absorbers” by spreading the load within the knee joint. Unfortunately, tears can occur within them with resultant pain or locking of the knee. These tears can be the result of sporting injuries or become more common with increasing age as the tissues lose their elasticity.
Knee arthroscopies or “scopes” are an excellent way of addressing these tears and allow trimming and smoothing of the torn cartilage. If the tear is large and is suitable for repair, then this can also be performed. Other conditions such as tears or defects in the joint surface or removal of loose bodies can also be dealt with.
Knee scopes are day procedures and are usually performed under a general anaesthetic. The actual procedure usually takes around 20 minutes with two small “key-hole” incisions which allow a camera to be placed within the knee and an instrument to be introduced that can address the pathology.
Patients are able to walk after the procedure and take 1-2 weeks off work. It usually takes 3-6 weeks to fully recover from a knee scope.
As with all surgical procedures, it is important to discuss the aims of surgery, benefits, as well as the possible risks.
Complications following surgery are rare but may include:
- anaesthetic problems
- bleeding into the joint
- blood clots
- injury to blood vessels or nerves
- swelling of the leg resulting from decreased blood flow
- post-operative infection
- very rarely, a knee ligament or cartilage may be slightly injured during surgery; this problem should heal without any further complication
Arthroscopy in general has a very low complication rate and it has certainly decreased problems overall compared to open surgery.
The experienced and cautious surgical team uses special techniques to minimise all the above risks. Adverse events following knee surgery are extremely rare, but they cannot be completely eliminated.
What to expect
Post operative course
Most patients go home a couple of hours after the procedure. You will note a bandage around the knee which covers water-proof dressings. Stitches are occasionally used but Steri-Strips (butterfly closures) are the most common method of closure. Local anaesthetic is often used so the knee is fairly comfortable in this period.
It is normal to expect some pain at night and you will be sent home with analgesics to cope with this. You are allowed to weight bear as tolerated and may require crutches. You will be given instructions for exercises and may be seen by a physiotherapist who will take you through these.
Driving can occur once you are mobile, comfortable and feel safe to control a vehicle.
Week 1
The bandage is taken off the next day and the knee is then covered with a Tubigrip (compression bandage) but with the dressings left intact.You are allowed to shower with these on as the dressings are waterproof. There may be some blood staining of the pads on the dressings; this is normal.
The dressings often fall off after 7-10 days.
Expect swelling and discomfort in the knee for up to 3-6 weeks post knee scope. Most patients find that their activity level increases significantly at the 3 week mark but may note that the knee responds to exercise with some inflammation (swelling).
Review
Review occurs at 2-3 weeks post-operation to discuss the findings of the procedure in detail, as well as to check that the knee is progressing well.
Total Knee Replacement
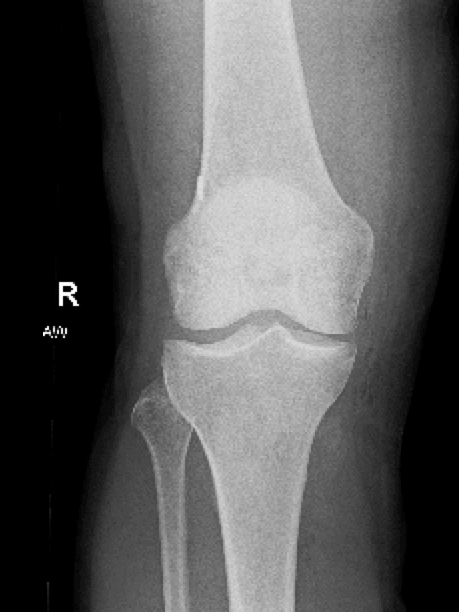
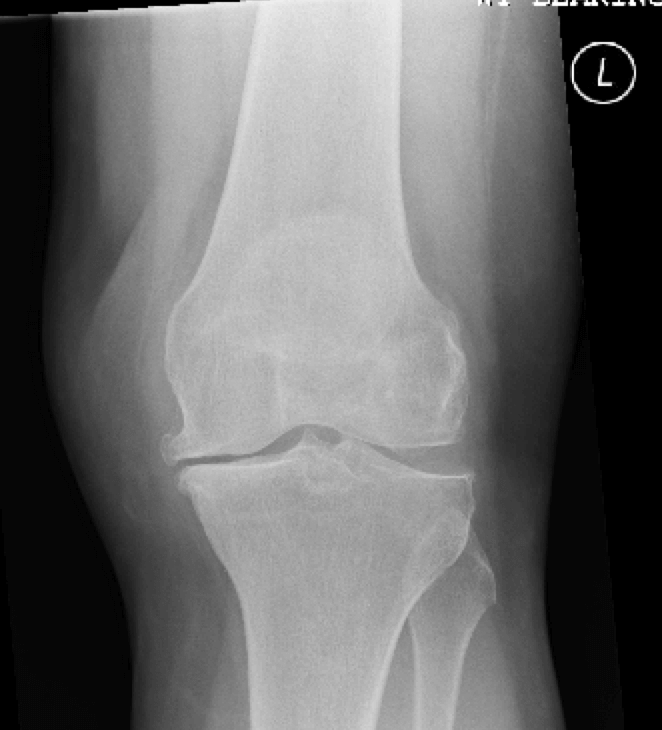
The numbers of total knee replacements (TKR) being performed yearly now exceed total hip replacements. This reflects how common knee arthritis is and how disabling it can be. Osteoarthritis is a degenerative condition which occurs when the joint cartilage covering the femur and the tibia wear away. This damage occurs over time but certain conditions like a previous knee injury or fracture can speed up the process.
Knee osteoarthritis presents with knee pain and stiffness which affects walking distance and activities of daily living. Night pain can be a major issue. Patients often note that their knees seem to appear more “bowed” or “knock-kneed.” This reflects progression of the disease.
The diagnosis is usually made on weightbearing x-rays but early changes can sometimes only be detected by MRI or a knee arthroscopy.

Initial management
Initial measures include activity modification such as avoiding impact activities like running, analgesics like Panadol Osteo (paracetamol) and anti-inflammatories like Nurofen (ibuprofen) or Mobic (meloxicam).
Procedure information
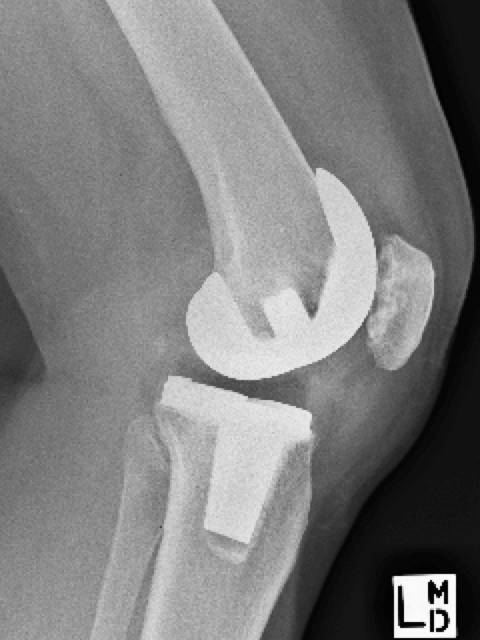
When conservative measures fail, it is then appropriate to consider a TKR. This operation involves replacing the worn joint surfaces and provides the benefit of reducing pain.
As TKR is major surgery, it is important to discuss the benefits and risks of surgery prior to making a decision to go ahead.
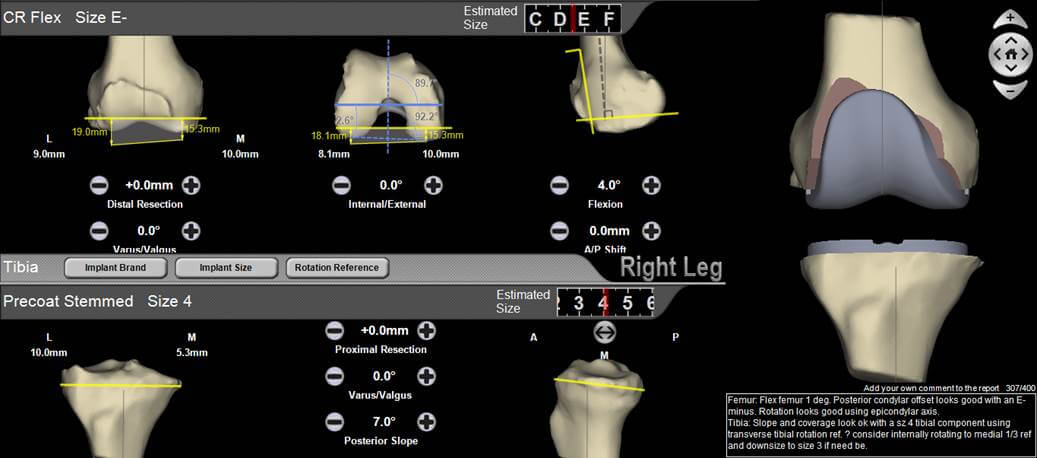
Knee replacements are performed using very accurate jigs in theatre but occasionally computer navigation or even patient specific jigs are used. In these settings, an MRI may need to be performed for planning purposes.
It is important for the patient to work hard on knee conditioning and range of motion post–operatively. This is extremely important in achieving the optimal result as one of the problems after a knee replacement can be loss of range of motion. Most patients find that it takes 3-6 months to recover fully from a total joint replacement.
Most complications are temporary setbacks. The results of knee replacements are generally considered to be excellent and the strong likelihood is that you will undergo the operation without any problems.
Some complications of total knee replacements include:
- blood clots
- postoperative infection
- loosening of the prosthesis from bone
- knee stiffness - this complication can be avoided by careful observance of post-operative instructions and rehabilitation protocols
- fracture
- residual pain and stiffness can occur
- leg length discrepancy
- damage to nerves or blood vessels
- allergy to the prosthesis (rare)
- anaesthetic issues
The experienced and cautious surgical team use special techniques to minimise all the above risks. Adverse events following knee surgery are extremely rare but they cannot be completely eliminated.

What to expect
How long will I be in hospital?
This procedure is a moderately large orthopaedic procedure and usually requires 4 to 5 days in hospital as well as a further in-patient period of rehabilitation.
When can I walk on the leg?
Patients are encouraged to get up and walk on the leg within 24 hours of your surgery. This may be aided with crutches or a frame; guided by our surgeon and physiotherapist.
Will I have a splint on my knee?
A Zimmer knee splint is sometimes used in the early post operative recovery period to aid in controlling the leg when walking. Your quadriceps muscles may be a little bit weak in the early post operative days requiring support. The knee splint can be discarded as soon as you can hold your leg straight against gravity.
What are the risks of surgery?
This operation, as with any others, requires an anaesthetic which in a fit, healthy young person is relatively straight forward. Specific anaesthetic risks will be discussed with your anaesthetist.
Risk of deep infection following this procedure is about one in 200. This is minimised by antibiotics given in your drip for 24 to 48 hours following your surgery.
A blood clot in the veins of the calf (deep venous thrombosis) is a potential risk but a blood thinning injection (heparin) will be given to you at the time of your operation to thin the blood enough to minimise this risk. If a blood clot should form, break off and go to the lungs, it can be serious and you must report any shortness of breath, coughing up of blood or severe chest pain. These are the signs of a pulmonary embolus.
What happens if I get an infection?
This is a major problem and may require further surgical procedures.
Will there be anybody else involved in my care?
Your surgeon has a strong team involved in managing your operation including a fully qualified consultant anaesthetist, surgical assistant and physician to help manage associated medical issues.
When can I drive?
Following a large procedure like this, a 6 week period will elapse before you are safe to drive. The key to the decision on driving is whether you can safely stop in an emergency situation. You can be guided by sitting in a stationary vehicle sitting in your driveway, imagining an emergency situation and attempting to make the appropriate avoidance procedures. If this is uncomfortable, you will know it is not safe to begin driving at this stage.
What is my prosthesis made from?
The prosthesis is made from a stainless steel metal alloy that is fixed to the bones with bone cement and impregnated with antibiotics to minimise infection risk. A polyethylene (plastic) bearing surface and spacer is attached to the tibial (shin bone) component to allow free movement between the components. The knee cap may need to be replaced when severe arthritis affects the kneecap as well.
Revision Total Knee Replacement
In some circumstances, a total knee replacement may have to be removed and revised.
Loosening
Knee replacements are mechanical devices with bearing surfaces that can wear out. This can result in wear particles components to loosen. A consequence of this can be bone loss and soft tissue damage. Fortunately, the modern knee replacement is proving to be very durable and early revisions for loosening are uncommon.
It is important to have your knee replacement checked if it is over a decade old and if you notice any change in function or develop pain.
If these knee replacements start to loosen then a revision knee replacement can be contemplated.
Infection
Another reason for revision knee replacement is infection. Unfortunately, one of the complications of a joint replacement is infection. This can either occur at the time of implantation or it can occur from bacteria lodging in the joint from the bloodstream. An infection in a joint replacement is serious and can cause the joint to fail or make the patient unwell.
If there is suspicion of infection, an urgent assessment is warranted. The knee may need to be investigated with blood tests, imaging and aspirations before definitive treatment.
An established infection may require the old components to be removed with placement of a temporary knee made of antibiotic cement. This is replaced with the definitive revision total knee replacement after a period of antibiotics.
Instability
Knee replacements are sometimes unstable with the ligaments sometimes being loose. Although they function very well, the design constraints of artificial joint replacements mean that they are unable to completely mimic the natural anatomy of the knee.
If the knee is unstable despite bracing and strengthening, then a revision to a more constrained knee may be considered.
Pain
10-15% of total knee replacements have ongoing pain. There can be issues with the alignment of the knee but in a majority of cases, no clear cause can be found. It is important to understand that revising a knee in these circumstances is generally not advisable unless a clear cause of pain has been identified.
A revision knee replacement is a bigger operation than a primary knee replacement. While the components may start to loosen, they are often still fixed to parts of the bone and removing them can be time consuming and risks removal of more bone. The operations are more complex, take more time and may involve a greater risk of blood loss, infection, fracture and damage to nerves and blood vessels.
It is important to discuss the case with your surgeon.
Patello-Femoral Joint
The joint that the kneecap (patella) forms with the groove in the distal femur is known as the patella-femoral joint. This can be a source of pain or instability from adolescence to elderly patients.
In the younger age group, the patella can cause anterior knee pain. This is relatively common in girls from 10-16 years of age and is usually accompanied by minimal findings on x-ray or MRI. The mainstay of management is physiotherapy.
Patello-femoral instability occurs when the knee cap dislocates laterally or outwards. The first episode usually occurs after a fall or sporting injury. This results in pain and swelling in the knee. It is important initially to make sure that the joint surface is intact and an x-ray and/or MRI may be required once the patella is put back in place in the emergency department. A short period of bracing followed by physiotherapy is usually required.
Recurrent instability can be a difficult problem to deal with. This can be caused by multiple factors including: laxity of the ligaments, the patella being placed too high (patella alta) or the femoral groove not being well formed (trochlea dysplasia). After careful assessment, a reconstruction of the medial patella-femoral ligament (MPFL) may be performed. This requires the use of the hamstring tendon to reconstruct the medial structures that help keep the patella in place. Another operation that may be performed is a tibial tubercle osteotomy. The tibial tubercle is the attachment point for the tendon that runs from the patella to the tibia. Changing the position of this can help the stability of the patella.
For all appointments and enquiries contact us on:
9:00am - 4:00pm Monday - Friday